Assessment of rehabilitation service outcomes: from patient to state
The ICF itself is only a classification that puts our understanding of, broadly speaking, human health in order [1]. However, this classification is based on a certain philosophy that generalizes modern ideas about health. How to use this philosophy in practice in rehabilitation and not to dig in the routine remains a big question. Currently, despite the widespread use of the ICF, its particular application causes many difficulties for specialists, as there are a lot of use cases and the interpretations of the classification.
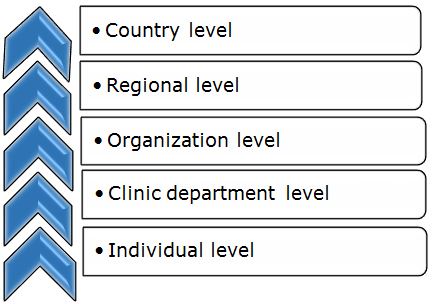
Modern ITs in health care facilitate many issues of documentation and allow to aggregate data from primary to managerial at the highest level (Chart 1). They directly change the technology of work, turning private agreements between specialists or organizations into a specialists’ joint space who can work on one task regardless of departmental affiliation and geographic location.
Chart 1: We can use ICF for assessment of rehabilitation services outcomes on the following levels
Basic data are persons and their needs. If specialists have certain skills, they can quite easily select those categories of ICF that reflect the health conditions of a given person. The choice of qualifiers for these categories, for comparability of results, should be determined by the most common methodologies in the country and the professional community. This will allow specialists of different qualifications and different professional views to come to the same results. The set of categories themselves is easier to choose from the ICF Core Sets [2] than from the full classification because they were specially selected for this case, which can also be used as a peculiar standard of assessment. Thus, we come to the categorical profile of the patient [3], which describes his health condition at the moment. Comparison of categorical profiles over time allows us to assess the dynamics of changes that occur in a person. Essentially, the qualifier is a normalized condition indicator, and accordingly, we can average these indicators and compare the average values if we have a need for integral dynamics. According to this technology, we can compare both the data of dynamics of one patient and the group of patients. This can be done both by the categorical profile as a whole, and by the categories defined to achieve the specific goal of rehabilitation.
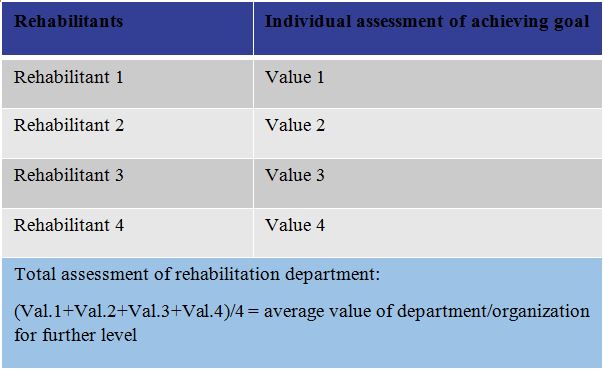
Comparing groups of averaged categorical profiles, we obtain a tool for assessing the effectiveness of teams of specialists or departments in an organization (Chart 2). However, here it is necessary to be correct when choosing data, to compare homogeneous data and avoid comparing and/or combining disparate entities, for example, comparing vocational rehabilitation with rehabilitation of people with spinal injuries.
Chart 2: The template of assessment of rehabilitation services on the individual level
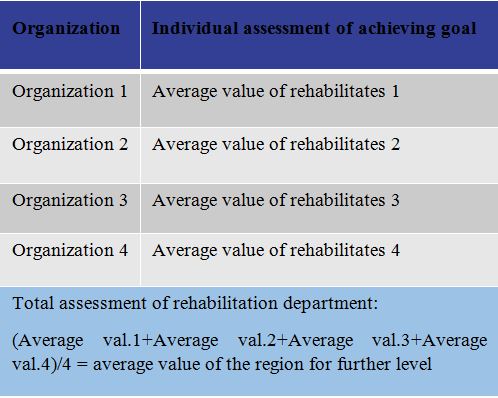
Having obtained the indicators of the work of departments, one can proceed to the assessment of the rehabilitation organization as a whole and, further, to a comparison of several rehabilitation organizations (Chart 3).
Chart 3: The template of assessment of rehabilitation services on the organization level
Thus, the ICF can become not only a classification that underlies the assessment of individual’s health condition, but also can be the basis for creating a tool for assessing the rehabilitation system at different levels of managing the rehabilitation system.
References:
1. International classification of functioning, disability and health : ICF. - World Health Organization 2001.- 299 p.
2. Bickenbach, J. ICF Core Sets (ISBN 9781616764319) / J. Bickenbach, A. Cieza, A. Rauch, [et al.] // Hogrefe Publishing, 2012.
3. Rauch, A. How to apply the International Classification of Functioning, Disability and Health (ICF) for rehabilitation management in clinical practice. / A. Rauch, A. Cieza, G. Stucki // EurJPhysRehabilMed. 2008;44(3):329–342
For information:
Alexander Shoshmin, Federal Scientific Centre of Rehabilitation of the Disabled n.a. G.A. Albrecht. Russia WHO-FIC Collaborating Centre, e-mail: shoshminav@mail.ru
Yanina Besstrashnova, Federal Scientific Centre of Rehabilitation of the Disabled n.a. G.A. Albrecht. Russia WHO-FIC Collaborating Centre, e-mail: besstjan@mail.ru
Victoria Lorer Federal Scientific Centre of Rehabilitation of the Disabled n.a. G.A. Albrecht. Russia WHO-FIC Collaborating Centre, e-mail: lorer@list.ru
Kristina Rozhko, Federal Scientific Centre of Rehabilitation of the Disabled n.a. G.A. Albrecht. Russia WHO-FIC Collaborating Centre, e-mail: rozhkokris@yandex.ru